







Please complete the inquiry form below. One of our staff will contact you within 1 business day
It keeps us upright, helps us carry much weight, and is equally flexible and stable. The human spine is an anatomical marvel that consists of millions of nerves that connect our brain to all nerves in the body. The spine is a highway for sending messages between the mind and body. Our spinal cord is protected by vertebrae bones that form the spine’s shape. Even a slight injury, loss of disc height, or degeneration of the back vertebrae or surrounding tissues can result in severe back pain.
DDD, or Degenerative disc disease, is an age-related medical condition diagnosed when one or more intervertebral discs (discs between the spinal column’s vertebrae) break down or deteriorate. Lower lumbar disc disease is often painful and can significantly impact a patient’s quality of life. Disc degeneration is a normal part of the aging process, and for many senior individuals, DDD isn’t an issue. For others, however, a degenerated disc may cause severe pain and chronic discomfort in the knee joints, back, hip joint, shoulder joint, and neck areas.
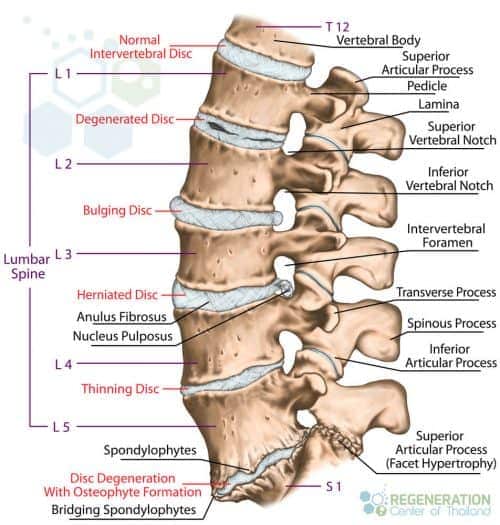
Degeneration of the spinal discs can happen for a variety of reasons. Simple events like walking, carrying heavy loads, repetitive movements, and shock-playing sports cause micro-injuries to our spinal column day after day. Often, these events go unnoticed, thanks to the vertebrae that act as shock absorbers. Every time the shock absorbers get used, a tiny amount of synovial fluid gets released to help “lubricate” the joints. During the sleep cycle, the discs can rebound to the initial stage. Still, over time, damage to chondrocytes and synovial cells from stress and inflammation causes this mechanism to lose effectiveness. This damage, over time, leads to asymmetric joint space narrowing, osteophytes, subchondral sclerosis, and cyst formations. A healthy spinal disc comprises a few parts, including the nucleus pulposus at the center of the spine and surrounded by the annulus fibrosus, a fibrous ring. The center nucleus pulposus area is a very soft, jelly-like, well-hydrated substance. Over time and with constant wear and tear, the nucleus pulposus (NP) begins to get stiff and dehydrated. This dehydration leads to a reduction in disc height & disc space narrowing, which causes excess stress on the annulus fibrosis. This stress damages the annulus, resulting in instability of posture and back pain. Such a scenario is diagnosed as intervertebral disc degeneration or DDD.
This spinal degeneration disease occurs slowly and gradually. Still, it is often felt first in the lumbar spine region because they are exposed to heavier loads more often than the discs in the neck (cervical spine) region. The spinal degeneration of intervertebral discs between the ( L5-S1) lumbar vertebra L5 and the lumbosacral segment S1 are most frequently affected. With symptomatic degenerative disc failure, chronic lower back pain radiates towards the hips, or often, there is a discomfort within the buttocks or thighs while walking; other symptoms, such as sporadic tingling or weakness in the knees might also be evident. Physical pain or discomfort might also be felt while bending, sitting, lifting, and twisting.
Chronic neck pain may also affect the upper spine. Patients often report discomfort or pain radiating to the arms, hands, and shoulders. The patients’ distress in the neck may interrupt healthy blood flow to the brain, consequently affecting memory and other cognitive skills. This interruption in the blood flow might also trigger headaches and vertigo.
Its location and stage of deterioration typically describe the severity of DDD:
Any back-related pain that is associated with intervertebral disc disruptions is referred to as “discogenic” pain. Depending on the severity of the disc bulge, the pain can be mild or very sharp. Some patients report feelings of lancinating, stabbing, or burning sensations, while others commonly report frequent numbness and tingling in extremities.
A herniated disc is also known as a bulged, slipped, or ruptured disc. This type of DDD occurs when the nucleus of a disc is pushed out of the center annulus into the spinal canal. This is typically caused by a rupture or tear rupture in the annulus ( fibrous ring), which causes pressure on the surrounding nerves and results in pain. About 90 percent of all cases of herniated disc failure occur in the lumbar spine region (lumbar disc herniation) but can also affect the thoracic spine (thoracolumbar) or sacrum (lumbosacral areas) of the spine. Risk factors that can increase the risk of having a herniated disk include Excess body weight, causing stress on the lower back discs. People with very physically demanding jobs also have a much higher risk of getting back problems. Unbalanced repetitive motions involving lifting, pushing, twisting, pulling, and bending sideways can also increase the risk of getting herniated disks. Genetics plays a part for some as people can inherit mutated genes that increase the risk of developing herniated discs.
To diagnose DDD and cervical degenerative disc disease, an orthopedic doctor examines the patient’s medical history and performs a physical examination. An MRI scan is often needed to identify areas of damage, but for patients
For the early stage of DDD or to manage the initial pain of degenerative discs, a combination of treatments is available, including:
Surgical treatment of DDD is another option for mild to severe degenerative disc disease but is usually recommended if nonsurgical therapies are ineffective. Surgery for Degenerative Disc Disease can result in additional complications ( failed surgery) or irreversible damage along with extended recovery periods requiring frequent rehabilitating that can affect daily life. Operations to treat DDD can include:
The artificial spinal discs are typically made up of:
Recovery from a total disc replacement surgery and pain relief can take 6-12 months and might require periodic spine adjustments to ensure successful grafting without additional complications.
When the discomfort and pain from degenerative spine & degenerative disc disease are severe, conventional operative therapies are often ineffective. Adult autologous stem cells can offer an innovative non-surgical therapeutic method to reverse bulging disc degeneration and address chronic low back pain at its root for these inoperative conditions. Chronic lower back pain due to degenerative disc illness impacts an estimated 200 million individuals worldwide. While short-term solutions can be achieved by the use of analgesics, steroids, having enough rest, and frequent physiotherapy, there are still many people diagnosed with discopathy whose conditions rapidly become worse despite the traditional treatments that orthopedic surgeons recommend.
If you are in this type of situation, you are often left with no other alternative but back surgery. The risky surgical method usually involves a spinal fusion or sometimes complete replacement of the degenerated disc with an artificial disc. Stem cell injections for back pain and MSC+ cell treatment for degenerative disk disease are currently the most reliable alternatives to back fusion surgery and contain endplate osteophytes.
The Regeneration Center offers cutting-edge cell-based treatments for spinal diseases such as DDD. The cellular approach is unique as it uses therapeutic levels of enhanced Mesenchymal stem cells (UC-MSC+ Cells.) These UC-MSC+ cells can differentiate into stem cells of the chondrogenic lineage. This lineage of cells is especially beneficial for patients with DDD for therapeutic cartilage regeneration. Isolated and enhanced UC-MSC+ cells can differentiate into chondrocyte cells and help to modulate the local areas of damage, support new growth, promote anti-inflammatory cytokines (pro-inflammatory cytokines), and enhance the body’s natural immunomodulatory functions. Stem cells for back pain & disc regeneration therapy offer an effective alternative to back surgery, which is disk regeneration using enhanced stem cells for pain management, helping heal and restore nerve sensations. The Regeneration Center offers the most advanced treatment for sports-related injuries, osteoporosis, sarcopenia and chronic degenerative disc disease. Our stem cell injections for back pain are much safer than invasive surgical procedures. They seek to treat the actual cause of the disease and reverse the condition through a targeted multi-step treatment to regenerate the damaged discs to their normal, healthy state.[1]
If you are currently experiencing slight to moderate discomfort or pain from a bulging disc or Herniated disc with lupus, you may be an ideal candidate for our innovative treatment, which uses proven and effective adult stem cell therapy to allow the spinal discs to regenerate without surgery.
The total number of cell infusions for DDD will depend on the patient’s needs. Most patients with mild to moderate DDD require multiple infusions of enhanced mesenchymal (UC-MSC+) cells per stage. Severe cases with multiple commodities may require several stages for sustained recovery.
Types of Stem Cells and Delivery Methods: For patients with moderate multi-level disc degeneration, multiple sessions of clinical grade expanded UC-MSC+ Mesenchymal Cells along with our proprietary mix of growth factors that can include Transforming Growth Factor-beta (TGF-β), Bone Morphogenetic Proteins (BMPs), Insulin-like Growth Factor-1 (IGF-1), Vascular Endothelial Growth Factors (VEGF), Fibroblast Growth Factors (FGF), Platelet-Derived Growth Factors (PDGF), Connective Tissue Growth Factors (CTGF), Epidermal Growth Factors (EGF), and Nerve Growth Factors (NGF). The regenerative therapy protocol will depend on the patient’s medical needs. Our autologous protocol will require 2-4 weeks of cell culturing before they can be used in therapies, while the allogeneic UC-MSC+ protocol does not require invasive surgeries or additional wait times. The isolated cells and growth factors are delivered via intravenous drips, direct local injections, intradiscal injections, intrathecal injections, fluoroscopy-guided stem cell delivery (in a hospital setting only), or a combination of different delivery methods to achieve the best results. To learn about the basics of stem cells, visit here.
Safety and efficacy are paramount; therefore, all clinical treatments for degenerative discs with stem cells require 1-2 Weeks in Bangkok, Thailand. Due to the varying degrees of spinal disc degeneration and injury experienced by each person, our orthopedic team will need to review medical records for all potential candidates before a detailed treatment protocol can be provided. Upon completion of treatment evaluation, a detailed plan will be provided, covering a day-by-day treatment calendar with all appointments, the exact number of days required, and the total medical-related costs (excluding accommodations or flights). To begin the treatment qualification process for our multi-stage DDD treatment in Bangkok, please prepare your recent medical records (MRI or CT Scans) and contact us today.
Post-Treatment Physical Rehabilitation & Pain Relief: Physical Rehabilitation after your treatment for DDD is optional, depending on your travel restrictions. Complete physical rehab is available for 2-4 hours per day and up to 5 days per week. Regenerative medical packages, medical visas, and extended stay accommodations for the patient and family/friends can also be provided upon request.
[1] ^ Sivakamasundari, V, and Thomas Lufkin. 2013. Stemming the Degeneration: IVD Stem Cells and Stem Cell Regenerative Therapy for Degenerative Disc Disease in Thailand. Advances in stem cells. doi:724547. https://www.ncbi.nlm.nih.gov/pubmed/23951558
[2] ^ Yang, Fan, Victor Y L Leung, Keith D K Luk, Danny Chan, and Kenneth M C Cheung. 2009. Mesenchymal stem cells arrest intervertebral disc degeneration through chondrocytic differentiation and stimulation of endogenous cells. Molecular therapy : The Journal of the American Society of Gene Therapy, no. 11 (July 7). doi:10.1038/mt.2009.146. https://www.ncbi.nlm.nih.gov/pubmed/19584814
[3] ^ Drazin, Doniel, Jack Rosner, Pablo Avalos, and Frank Acosta. 2012. Stem cell therapy for degenerative disc disease. Advances in orthopedics (April 24). doi:10.1155/2012/961052. https://www.ncbi.nlm.nih.gov/pubmed/22593830